







Why 911 Can't Save You From Choking: The 4-Minute Truth Every Family Must Know
Quick Answer: When someone chokes, brain damage begins at 4-6 minutes without oxygen, and death follows by 8-10 minutes. Yet the average US EMS response time is 7 minutes in urban areas, 14+ minutes in rural areas, with 1 in 10 emergencies waiting nearly half an hour. By the math, 911 mathematically cannot save most choking victims — bystander or self-rescue is the only realistic intervention within the critical window. This is why federal agencies created the "Until Help Arrives" campaign, why emergency medical professionals increasingly keep anti-choking devices in their own homes, and why the NovaCare Anti-Choking Device ($63.98) — Bureau Veritas Tested with verified 70 kPa suction — exists. Save #156 and Save #162 are documented cases where self-rescue happened in seconds, hours before EMS could have arrived. This guide explains the brutal math of choking emergencies and what every family must do before 911 is needed.
You've been told your whole life to "call 911" in an emergency.
For choking, that advice is mostly fiction.
Not because 911 doesn't work — it does, brilliantly, for heart attacks, strokes, falls, and a hundred other emergencies. But choking operates on a clock that 911 simply cannot match. By the time the dispatcher answers, your brain has already begun the dying process.
This isn't paranoia. This is mathematics. And it's the conversation every family must have before they need it.
Section 1: The Brutal Mathematics (5 Questions)
Q1: How long does someone have during a choking emergency?
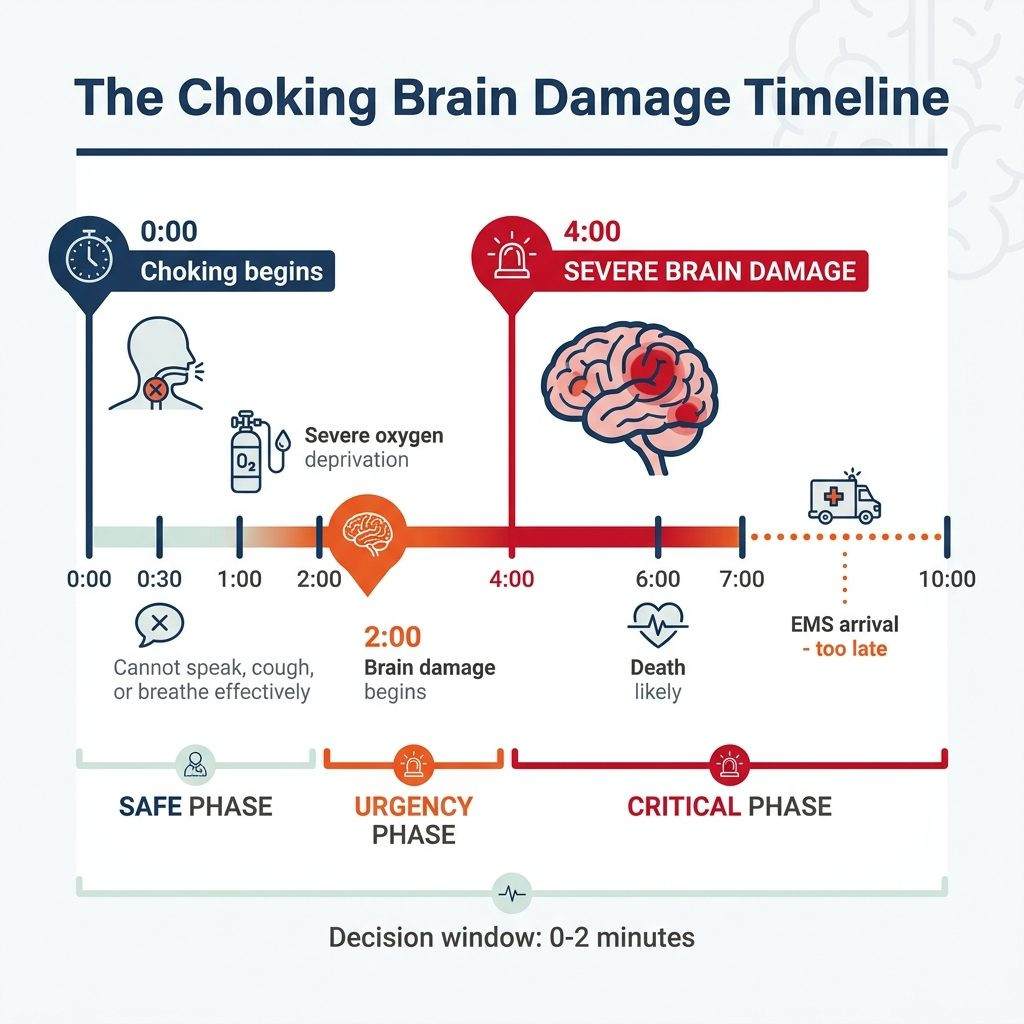
The neurological clock is unforgiving:
- 0-30 seconds: Realization, attempts to cough, panic begins
- 30-60 seconds: Cannot speak, cannot scream for help
- 1-2 minutes: Severe oxygen deprivation, loss of consciousness possible
- 2-4 minutes: Brain damage begins (irreversible)
- 4-6 minutes: Severe, permanent brain damage
- 6-10 minutes: Death likely without intervention
This is documented across multiple peer-reviewed neurological studies. The brain — which uses 20% of the body's oxygen despite being only 2% of body weight — cannot tolerate prolonged hypoxia.
The critical decision window: 0-2 minutes. After that, even successful rescue may leave permanent neurological damage.
Q2: What is the actual average EMS response time in the United States?
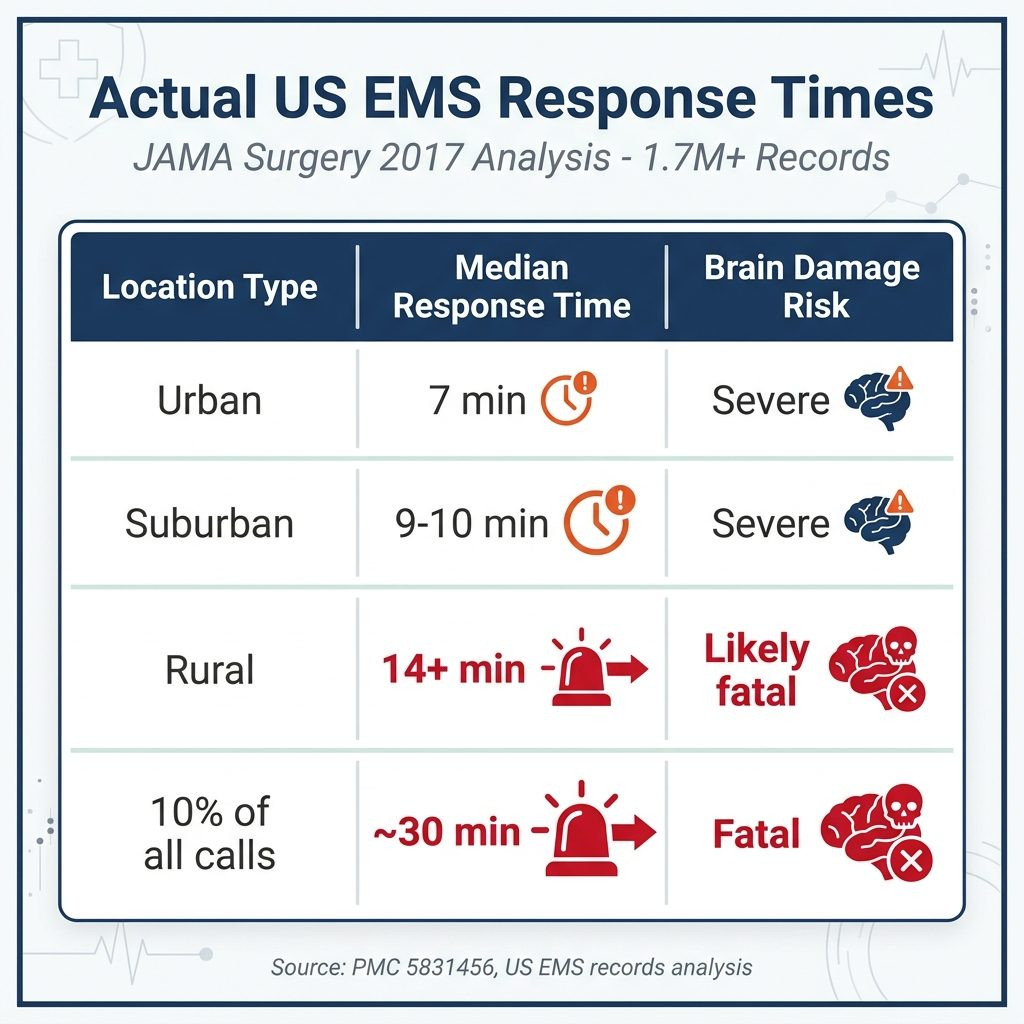
Per a comprehensive 2017 analysis published in JAMA Surgery (PMC 5831456), examining over 1.7 million EMS records:
| Location Type | Median Response Time | Brain Damage Risk |
|---|---|---|
| Urban (population > 50,000) | 7 minutes | Severe |
| Suburban (2,500-50,000) | 9-10 minutes | Severe |
| Rural (< 2,500) | 14+ minutes | Likely fatal |
| 10% of all calls | ~30 minutes | Fatal |
The math is stark: even in optimal urban conditions with the fastest EMS response in the world, EMS arrives after brain damage has already begun.
Note: NFPA 1710 standard sets 4 minutes for first responder arrival and 8 minutes for ALS (Advanced Life Support). These are targets, not guarantees, and they require 90% reliability — meaning 10% of cases exceed these times.
Q3: Why can't EMS arrive faster?
Multiple factors create the time gap:
- Call processing time: 30-90 seconds for dispatcher to gather information
- Crew preparation: Locate vehicle, route mapping
- Traffic conditions: Even with sirens, traffic delays
- Geographic distance: Especially in rural areas
- Building access: Apartment buildings, gated communities
- Multiple casualty events: Resources may be dispatched elsewhere
The 911 system is designed for a wide range of emergencies. For choking specifically, even a "fast" response is too slow.
Q4: What does the federal government say about this?
The US Departments of Homeland Security, Defense, and Health & Human Services jointly created the "Until Help Arrives" campaign (community.fema.gov/until-help-arrives) precisely because EMS response times often exceed the survival window for time-critical emergencies.
The campaign's core message: bystanders and individuals must be prepared to act in the minutes before EMS arrives. For choking, "acting" traditionally meant Heimlich maneuver. But Heimlich requires another conscious person — and even when present, has documented failure rates of 20-25%.
The federal government has, in effect, acknowledged that 911 alone is insufficient for time-critical emergencies. They're asking citizens to be the first responders.

Q5: How often does choking actually result in death because of response time?
Per CDC data:
- 5,000+ choking deaths annually in the United States
- 4th leading cause of accidental death in adults 65+
- 45% of choking deaths happen at home (San Diego County study)
- Adults 65+ die at 8x the rate of younger adults
The majority of these deaths involve people who would have survived if intervention occurred within the critical window. The intervention didn't come because no one was equipped to provide it before EMS arrived.
Section 2: Why Heimlich Often Fails (5 Questions)
Q6: Doesn't Heimlich work if someone knows it?
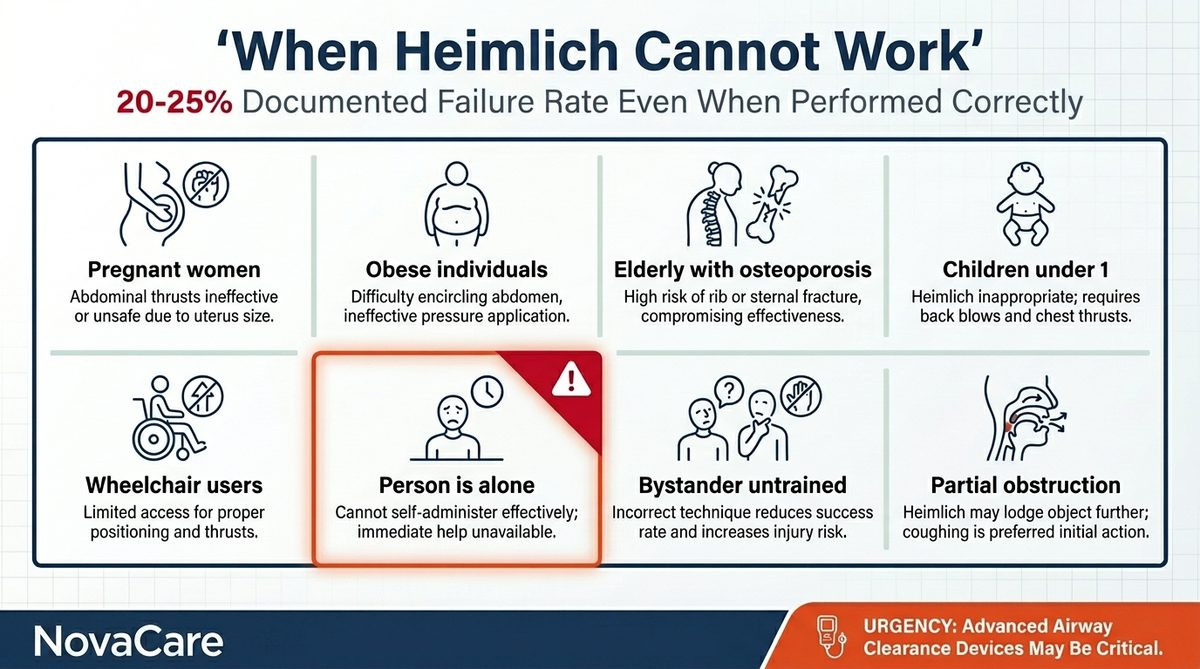
Heimlich (abdominal thrust) works in many cases — but not all. Documented failure scenarios:
- Pregnant women — Cannot use abdominal thrust
- Obese individuals — Difficult to perform effectively
- Elderly with osteoporosis — Risk of rib fracture
- Children under 1 — Different technique required (back blows)
- Wheelchair users — Positioning challenges
- Person is alone — Self-Heimlich rarely successful
- Bystander has no training — Frequent failure
- Object is partial obstruction — Heimlich may not dislodge
Per emergency medicine research, Heimlich has documented failure rates of 20-25% even when performed correctly. The "fail" outcome typically means continued obstruction and death.
Q7: Can someone perform Heimlich on themselves?
Theoretically yes, practically often no:
- Requires recognizing situation in time (panic interferes)
- Requires finding suitable surface (chair back, counter edge)
- Requires sufficient strength to thrust effectively
- Requires repeating multiple times with declining strength
- Often unsuccessful — coordination impaired by hypoxia
For elderly individuals — particularly those with arthritis, balance issues, or living alone — self-Heimlich is rarely a viable option. This is precisely why 27% of seniors who live alone face unique vulnerability.
Q8: What if there's a bystander but they don't know Heimlich?
This is unfortunately common:
- Only ~40% of Americans have ever received CPR/first aid training
- Of those, many have not refreshed training in 5+ years
- Recognition of choking signs is delayed in panic
- Untrained bystanders often hit back (wrong), give water (wrong), etc.
The result: even with bystanders present, choking events often progress unchecked because the bystanders don't know how to help effectively.
Q9: What about choking at restaurants — surely staff can help?
Restaurant staff training varies dramatically:
- Most states don't require choking response training
- Staff turnover means many haven't trained recently
- Manager may have training but not on-floor staff
- Even trained staff freeze in real emergencies
- Time to identify, respond, and act often exceeds critical window
Some states (Massachusetts, others) have begun requiring anti-choking devices in restaurants. The fact that legislation is needed proves restaurants can't reliably handle choking through training alone.
Q10: What about hospitals and care facilities?
Care facilities have higher response capability than homes, but still face challenges:
- Staff-to-resident ratios mean delays
- Even on-site nurses must reach the resident
- Recognition time depends on visibility
- Equipment may not be immediately accessible
- Multiple residents may be eating simultaneously
Per nursing home studies, choking events in long-term care facilities still have significant mortality despite trained staff being present. Choking moves faster than humans.
Section 3: What Emergency Professionals Actually Do (5 Questions)
Q11: Do EMS professionals keep anti-choking devices at home?
An increasing number do. The reasoning is straightforward:
- They've responded to choking calls and seen response time delays firsthand
- They understand the 4-minute brain damage window better than civilians
- They know Heimlich's failure scenarios from experience
- They have families they want to protect
- They've seen what successful suction-based devices accomplish in their own work
EMS personnel use suction devices routinely in their professional work. Many have extended this same principle to their personal household preparation — keeping appropriate suction-based anti-choking devices at home.
This isn't a marketing claim. It's a logical pattern emerging among professionals who understand emergency response from inside.
Q12: What do firefighters and police say?
First responders across multiple disciplines share similar perspectives:
- Firefighters: Often arrive first (NFPA 1710 standard) but lack hospital-grade suction equipment
- Police: May arrive first but typically have no choking-specific equipment
- EMTs: Best equipped but arrive 7+ minutes later on average
The gap between "first on scene" and "equipped to handle choking" is the dangerous middle ground. Modern anti-choking devices fill that gap by allowing immediate action by anyone present.
Q13: How do anti-choking devices fit into emergency response training?
Modern emergency response training increasingly includes:
- Recognition of choking emergency
- Initial response (encourage cough, abdominal thrust)
- Anti-choking device use as escalation
- Calling 911 in parallel (not instead of)
- Continued attempts until EMS arrival
The protocol acknowledges what older training didn't: equipment-based interventions extend the window between failed first attempts and EMS arrival. This window is often the difference between life and death.
Q14: How do anti-choking devices work mechanically?
The principle is suction — generating negative pressure to dislodge the obstruction:
- Mask seals over mouth (and sometimes nose)
- Activation creates suction force
- Suction pulls obstruction toward the device, away from airway
- Object exits when freed from airway tissue
- Reusable devices allow practice and repeated attempts
NovaCare's mechanical design generates up to 70 kPa suction (independently verified by Bureau Veritas, Report BV2500728QN7119) — sufficient to dislodge most food obstructions on first attempt.
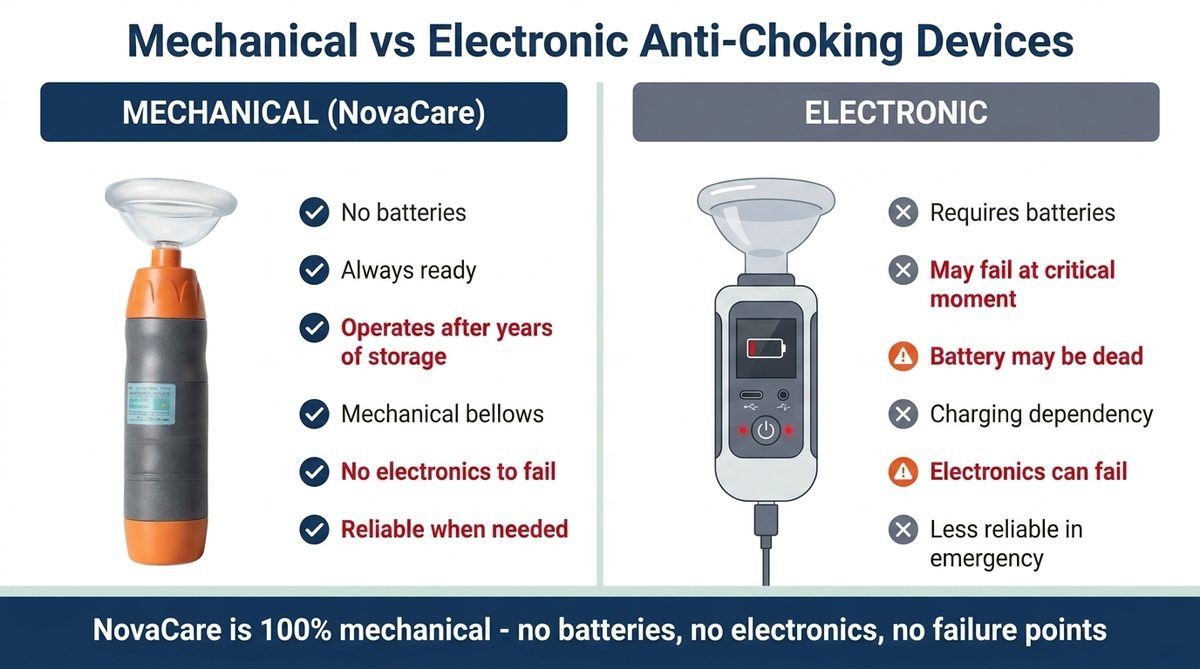
Q15: What's the difference between mechanical and electronic anti-choking devices?
Critical distinction:
- Mechanical devices: Use spring, plunger, or bellows mechanism. No batteries. Always ready. Operate even after years in storage.
- Electronic devices: Require batteries or charging. Failure mode at critical moment. May not work after long storage.
NovaCare is fully mechanical. There are no batteries, no electronics, no parts that degrade with time. When you need it — even five years after purchase — it works exactly the same as day one.
This matters because anti-choking devices live in drawers. They're rarely used. They must work reliably when called upon, often after years of storage.
Section 4: Why Self-Rescue Capability Matters Most (5 Questions)
Q16: Why is self-rescue capability the most important feature?
Self-rescue addresses the fundamental gap: when no one else is present or capable.
Statistics requiring self-rescue:
- 27% of Americans 65+ live alone (US Census)
- Even with cohabitants, many household members may be in other rooms, asleep, in shower
- Choking often happens during routine activities (eating, snacking)
- Many choking events are silent — no time for others to notice
If a device requires another person to operate it (like LifeVac), it provides no protection during solo moments. Self-rescue capable equipment provides protection across all scenarios.
Q17: Has self-rescue actually been documented to work?
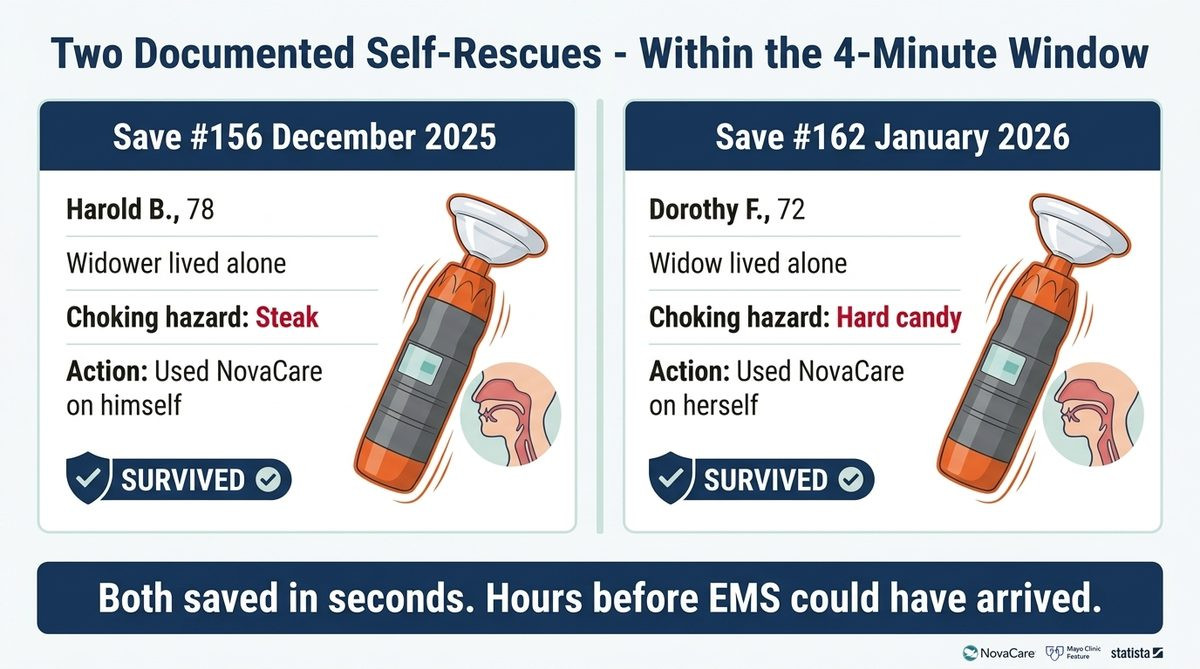
Yes — NovaCare has documented self-rescue cases:
Save #156 (December 2025):
- Harold B., 78 years old
- Choking on steak, alone in kitchen
- Tuesday-night dinner routine
- Used NovaCare on himself
- Cleared in seconds
- Survived
Save #162 (January 2026):
- Dorothy F., 72 years old
- Choking on hard candy, alone watching TV
- Used NovaCare on herself
- Object cleared
- Survived
Both cases occurred within the 0-2 minute critical window. Both seniors used the device WITHOUT any other person present. Both survived hours before EMS could have realistically arrived.
This is what self-rescue capability actually looks like in practice.
Q18: What makes a device truly self-rescue capable?
Critical design requirements:
- One-handed operation — Other hand may need stabilization
- Single-button activation — Coordination impaired during hypoxia
- No assembly required — Brain function reduced
- Mechanical reliability — Works without preparation
- Compact size — Within arm's reach
- Forgiving operation — Works with imperfect technique
- Reusable for practice — Muscle memory development
Most anti-choking devices were designed for bystander use, not self-rescue. NovaCare was specifically designed to meet all self-rescue requirements.
Q19: Where should the device be kept to be useful?
"Within arm's reach" is the operating principle:
| Location | Why Essential |
|---|---|
| Kitchen counter | Food preparation, snacking |
| Dining area | Where most meals happen |
| Living room (next to TV chair) | Snacking while watching TV |
| Bedroom nightstand | Late-night eating |
| Travel bag/car | Restaurants, road trips |
Devices stored in cabinets, attics, or "somewhere upstairs" provide no protection during the 4-minute window. The 2-pack pricing ($119.98 for two) makes multi-location placement affordable.
Q20: How does practice with a device save real time?
Hypoxia impairs:
- Cognitive function
- Fine motor coordination
- Problem-solving capability
- Reading instructions
If the first time someone uses the device is during a choking event, valuable seconds disappear into figuring out the operation. Pre-practiced muscle memory takes over when conscious thinking falters.
NovaCare's reusable design enables practice. Families can demonstrate together. Children old enough can practice on family pets' toys. Muscle memory at the moment that matters.
Section 5: The Family Action Framework (5 Questions)
Q21: What should every family do today?
The "before you need it" checklist:
- Acknowledge the math — 4-minute brain damage window vs 7+ minute EMS response
- Identify vulnerable family members — Children under 5, adults over 65, those with swallowing conditions
- Acquire anti-choking equipment — Mechanical, self-rescue capable, in primary eating areas
- Practice as a family — Everyone shown how to use device
- Practice Heimlich basics — Still useful as first intervention
- Strategic placement — Not in drawer, within arm's reach
- Communication plan — Who calls 911 while who uses device
- Refresh annually — Brief family review each year
Q22: Should we still call 911 if using an anti-choking device?
YES — always. Even if the device works perfectly:
- Choking events may have caused unseen tissue damage
- Aspiration pneumonia risk after event (24-72 hour window)
- Some objects may have been pushed deeper rather than out
- Medical evaluation needed to confirm complete clearing
- Witness/documentation for follow-up care
Use the device immediately, call 911 in parallel (or have someone else do it). EMS can verify successful intervention and transport for evaluation.
Q23: How do I balance fear-mongering vs preparation?
This is a real concern — families don't want to spend daily life in fear.
The reframe: equipment readiness eliminates fear rather than creating it.
- Smoke detectors don't make you fear fire
- Fire extinguishers don't increase fire anxiety
- Car seat belts don't increase crash worry
- Anti-choking devices don't increase choking fear
Once equipped, the question "what would we do if X happened?" is answered. The mental anxiety often associated with parenting young children or aging parents lifts. Preparation enables peace, not paranoia.
Q24: What if my family member refuses to take this seriously?
Common responses and approaches:
"I'm not going to choke"
- Reply: "We don't expect to need smoke detectors either. That's the point."
- Reference: 5,000+ Americans die yearly. Many had said the same thing.
"You're being paranoid"
- Reply: "EMS response time is 7+ minutes. Brain damage starts at 4. That's not paranoia, that's math."
"My doctor never mentioned this"
- Reply: "Doctors don't routinely cover home emergency equipment. This isn't medical advice — it's emergency preparedness."
"It's too expensive"
- Reply: "$63.98 once. Less than a single tank of gas. Less than dinner for two."
Q25: What's the cost of not preparing?
Per family economics:
- Anti-choking device: $63.98 (one-time)
- 2-pack for two locations: $119.98 (one-time)
- Family practice session: 30 minutes (one-time)
- Annual refresh: 5 minutes
Versus the cost of preventable choking death:
- Immediate family devastation
- Funeral and related costs ($7,000+ average)
- Long-term grief and psychological impact
- "What if we had been prepared?" — endless rumination
The expected-value calculation overwhelmingly favors preparation. The asymmetry between cost and consequence is extreme.
For Every Family: A Letter to You
You've been told 911 will save you in an emergency. For most emergencies, it will.
For choking, it almost certainly won't — not because 911 is failing, but because choking outruns even the fastest emergency response.
This isn't a marketing message. It's the documented reality acknowledged by the same federal agencies that built the 911 system. They created the "Until Help Arrives" campaign specifically because they know EMS can't always arrive in time. They're asking families to be the first link in the chain of survival.
For choking, that means:
- Recognize the math — 4 minutes for brain damage vs 7+ minute response
- Acknowledge that traditional methods (Heimlich) have documented failure rates
- Prepare with equipment designed for the actual scenarios you face
- Practice so muscle memory exists when conscious thought falters
- Place equipment within arm's reach of where eating happens
- Train every family member capable of using it
Save #156 was a Tuesday-night dinner. Save #162 was an evening of watching TV with hard candy. Both happened in homes where, statistically, EMS would have arrived after brain damage had already begun.
Both survived because the device was within reach, because they'd seen how to use it, because the device was mechanical and ready, because no batteries were dead, because no app needed updating, because nothing required setup.
One button. One hand. Pressed in time.
That's the entire technology. That's the entire training. That's the difference between "EMS arrived too late" and "thank God I had that thing."
→ Get NovaCare Before You Need It — $63.98 single · $119.98 2-pack
The 2-pack covers kitchen + bedroom or kitchen + living room.
The Bottom Line
Average US EMS response time is 7 minutes urban, 14+ minutes rural. Brain damage from choking begins at 4-6 minutes. The math means 911 mathematically cannot save most choking victims acting alone. Bystander or self-rescue is the only viable intervention within the survival window. Federal agencies acknowledge this through the "Until Help Arrives" campaign. Emergency professionals increasingly keep anti-choking devices in their own homes for the same reasons.
- ✅ Bureau Veritas Tested (Report BV2500728QN7119)
- ✅ 70 kPa Medical-Grade Suction (Independently Verified)
- ✅ IP65 Rated (Dust & Water Resistant)
- ✅ CE & UKCA Certifications In Progress
- ✅ 20 Documented Saves in 2026
- ✅ 2 Senior Self-Rescues (#156, #162)
- ✅ Reusable Design (Not Single-Use)
- ✅ Mechanical One-Button (No Batteries)
- ✅ Self-Rescue Capable
- ✅ $63.98 single · $119.98 2-pack
- ✅ Free US Shipping
- ✅ 90-Day Money-Back Guarantee
→ Get NovaCare at novacareus.com
📖 Related: Anti-Choking Device for Seniors: 30 Questions Answered
📖 Related: Choking While Alone: Solo Senior Safety
📖 Related: Heimlich Maneuver: Step-by-Step Guide
📖 Related: Signs of Choking: Recognize It in 5 Seconds
📖 Related: NovaCare 2026 Lives Saved Report