







Dentures and Choking Risk: Why Your Parent's False Teeth Are a Hidden Danger
Quick Answer: Dentures dramatically increase choking risk in ways most families never consider. Per peer-reviewed research, denture wearers experience significantly reduced oral sensation, impaired swallowing function (videofluoroscopic swallowing studies show measurable differences with vs. without dentures), and 2.37x higher odds of moderate-to-severe airflow limitation (PRIME study, PMC 10194954). With ~40 million American adults wearing dentures — most over 65 — this represents an enormous under-recognized choking risk population. The NovaCare Anti-Choking Device ($63.98) — Bureau Veritas Tested with verified 70 kPa suction — provides emergency response when denture-related swallowing impairment leads to choking. Save #156 (Harold B., 78) and Save #162 (Dorothy F., 72) document senior self-rescue success. Adult children of denture-wearing parents need to understand this hidden risk.
Your mother got her dentures fifteen years ago. She's adapted beautifully — eats almost everything, smiles confidently, never complains.
You assume the dentures are simply replacements for teeth. They are. But they're also altering her swallowing in ways neither she nor her dentist may have discussed with you.
This guide explains the documented research on dentures and choking risk, the high-risk foods most denture wearers don't know to avoid, and what adult children of denture-wearing parents need to do.
Section 1: The Hidden Mechanics of Denture-Related Risk (5 Questions)
Q1: How do dentures actually increase choking risk?
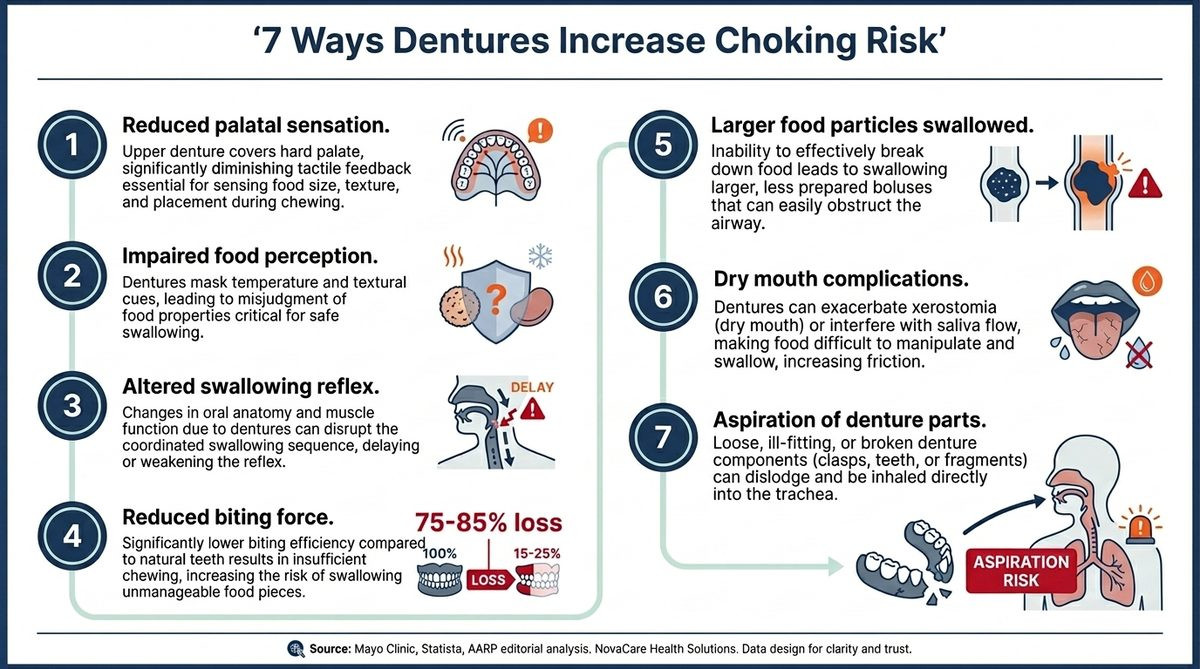
Multiple documented mechanisms working together:
- Reduced palatal sensation — Denture covers the hard palate, blocking sensation
- Impaired food perception — Cannot feel food size/temperature/texture as accurately
- Altered swallowing reflex — Documented changes in oral transit time
- Reduced biting force — Approximately 1/4 the force of natural teeth
- Larger food particles swallowed — Inadequate chewing leads to bigger pieces
- Dry mouth complications — Many denture wearers experience reduced saliva
- Aspiration of denture parts — Loose dentures can dislodge during eating/sleep
The combination creates compounding risk that most denture wearers — and their families — never consider.
Q2: What does research say about denture wearers and swallowing?
Per a peer-reviewed videofluoroscopic swallowing study (PMC 3660487):
- Researchers examined 24 patients with removable dentures
- Compared swallowing function with dentures in vs. removed
- Found measurable changes in oral transit time (OTT)
- OTTs were significantly different when dentures were worn vs removed
- Statistical significance confirmed across the study population
This is the kind of documented evidence most denture wearers never see. The very act of wearing dentures alters the mechanical reality of swallowing.
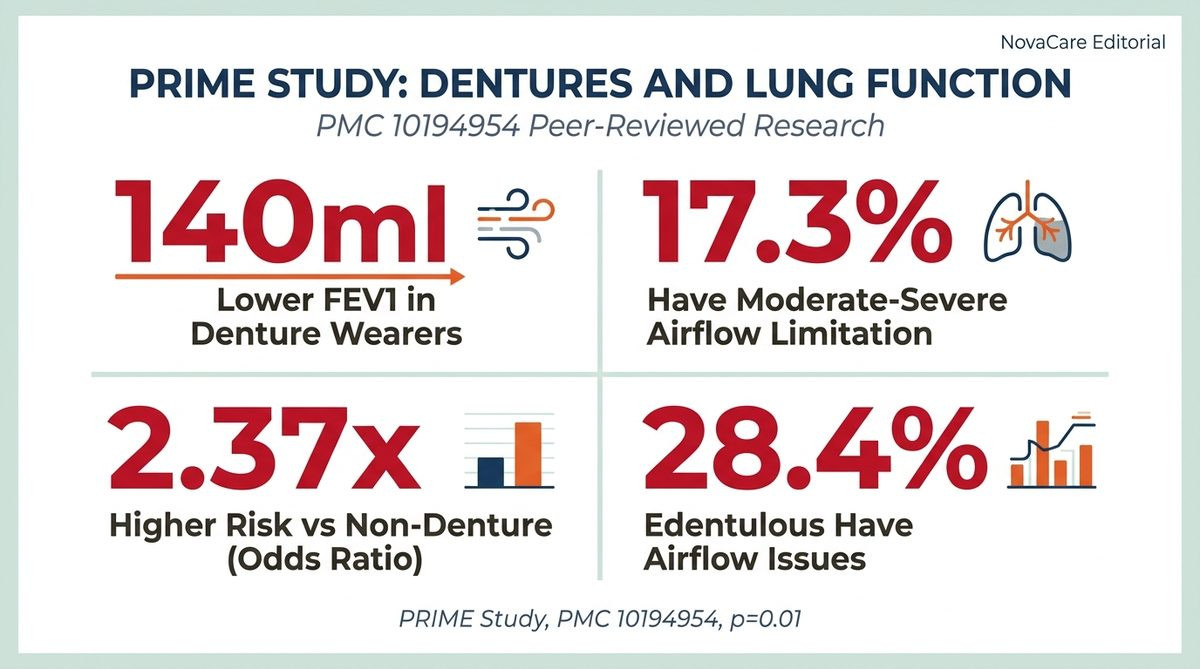
Q3: Do dentures affect lung function too?
Yes — per the PRIME study (PMC 10194954) examining 353 partially dentate men aged 58-72:
- Denture wearers had FEV1 (forced expiratory volume) averaging 140ml lower than non-denture controls
- 4% reduction in percent predicted FEV1 (p=0.0022)
- 17.3% of denture wearers had moderate-to-severe airflow limitation vs 9.3% of controls
- Adjusted odds ratio: 2.37x higher risk for moderate-to-severe airflow reduction (p=0.01)
- Edentulous men (no natural teeth) had even higher rates: 28.4% with airflow limitation
The lung function reduction matters for choking response: when choking happens, cough strength is critical for clearing partial obstructions. Denture wearers have compromised cough capacity to begin with.
Q4: Why does palatal sensation matter so much?
The hard palate (roof of mouth) is critical for safe eating:
- Detects food size before swallowing
- Senses temperature (prevents burns)
- Identifies food texture (firm vs soft)
- Triggers chewing reflexes
- Coordinates swallowing initiation
- Detects foreign objects (bone chips, pits)
When dentures cover the palate (especially upper dentures), this entire sensory system is blocked or significantly impaired. The senior literally cannot feel what's in their mouth the way someone with natural teeth would.
The implication: they may attempt to swallow food that's too large, too tough, or contains hidden hazards (small bones, fruit pits, hard fragments) because they cannot sense the problem in time.
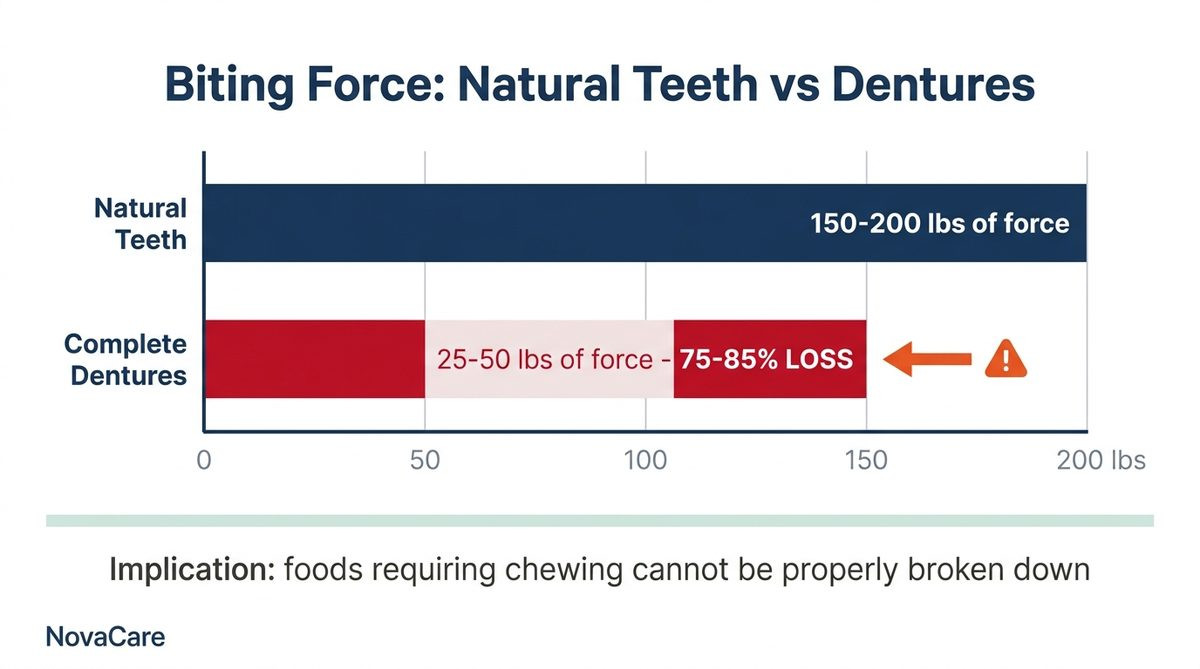
Q5: How much chewing force is lost with dentures?
The numbers are stark:
- Natural teeth: 150-200 pounds of biting force
- Complete dentures: Approximately 25-50 pounds of biting force
- Reduction: Approximately 75-85% loss of biting force
This means foods that require significant chewing (steak, tough vegetables, nuts, hard candies) cannot be properly broken down before swallowing. Larger food particles travel down the throat — increasing obstruction risk.
Per peer-reviewed denture research, swallowed food particle sizes are measurably larger in denture wearers compared to natural teeth controls.
Section 2: High-Risk Foods for Denture Wearers (5 Questions)
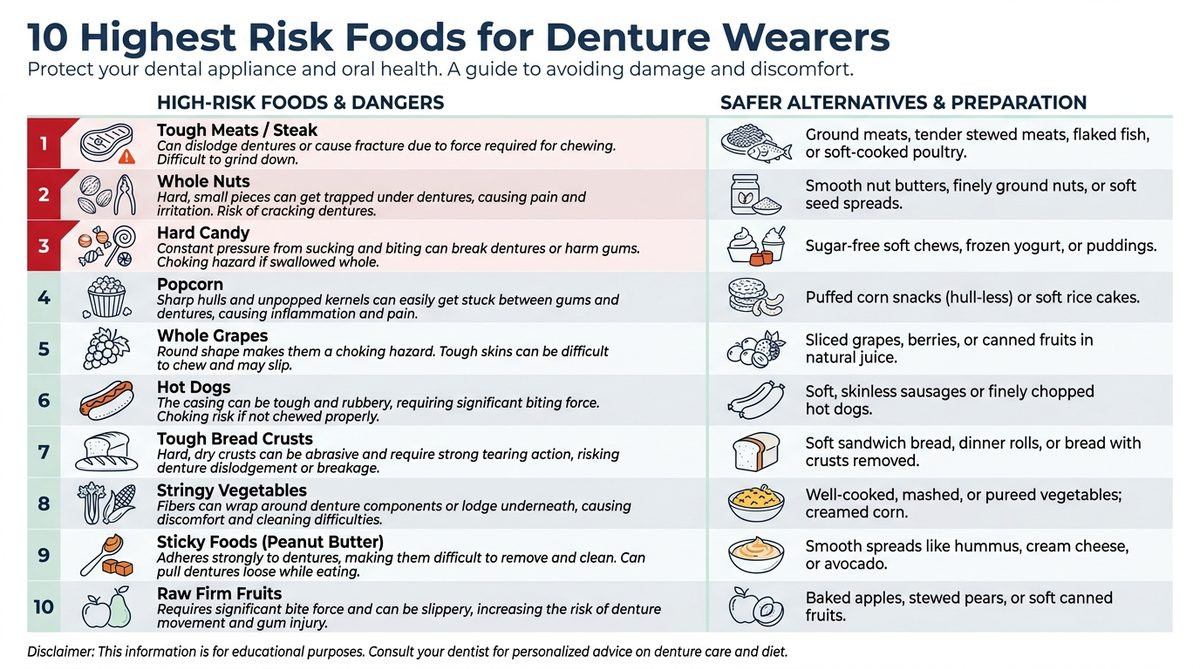
Q6: Which foods pose the highest choking risk for denture wearers?
Per gerodontology research and senior care literature:
| Food Category | Why High Risk for Dentures | Safer Alternative |
|---|---|---|
| Tough meats (steak, jerky) | Cannot chew adequately | Slow-cooked, ground, or fish |
| Whole nuts | Small, smooth, perfect plug shape | Nut butter, ground nuts |
| Hard candy | Cannot be chewed, slick surface | Soft candy or skip entirely |
| Popcorn | Hulls cannot be felt with dentures | Avoid entirely |
| Whole grapes | Smooth surface, plug shape | Quartered |
| Hot dogs (whole) | Smooth, round, perfect obstruction | Sliced lengthwise + small |
| Tough bread crusts | Requires significant biting force | Soft bread, no crust |
| Stringy vegetables (celery) | Cannot break fiber strands | Cooked until soft |
| Sticky foods (peanut butter) | Adheres to dentures | Thin spread, with bread |
| Raw firm fruits (apple) | Hard texture overwhelms biting force | Sliced thin or cooked |
Q7: What about fish bones — are they more dangerous with dentures?
Significantly more dangerous. Why:
- Small fish bones are typically detected by palatal sensation
- With dentures covering the palate, bones cannot be felt
- Bones get swallowed inadvertently
- Can lodge in throat or esophagus
- May cause perforation requiring surgery
For denture-wearing seniors, consider:
- Boneless fish only
- Pre-portioned fish (salmon fillets without skin)
- Visual inspection of every bite
- Avoid bony fish (trout, mackerel, bony cuts of salmon)
Q8: Are some foods particularly dangerous when dentures are loose?
Yes — and many seniors have loose dentures without realizing the severity:
Loose dentures create additional risks:
- Movement during chewing — food gets pushed wrong direction
- Denture itself can shift into throat
- Sticky foods can pull dentures partially out
- Air gaps reduce suction (loose feel)
- Eating speed unconsciously increases
If your parent's dentures click, shift visibly while talking, require frequent adjustment, or have caused them to switch to soft foods only — they need a denture reline or replacement immediately. Loose dentures aren't just uncomfortable, they're a choking hazard.
Q9: Can dentures themselves cause choking?
Yes, multiple documented mechanisms:
- Partial dentures with metal clasps — Can detach and become airway obstruction
- Broken denture fragments — Particularly during eating hard foods
- Loose complete dentures — Can shift into throat during sleep
- Denture-aspiration during anesthesia — Should always be removed before surgery
Per case reports in medical literature, denture aspiration is a documented emergency requiring immediate intervention. Many denture aspiration events occur in:
- Sleep (dentures should be removed before sleep)
- Surgical/anesthesia situations
- Seizures or syncope events
- Dementia patients who don't recognize loose dentures
Q10: What about adhesives — do they help reduce risk?
Denture adhesives help with retention but have their own considerations:
Benefits:
- Better retention reduces shifting during eating
- Improved chewing confidence
- Less air gap between denture and gum
- Per research (PMC 9714889), adhesive use can reduce oral impacts
Concerns:
- Excessive use may indicate poorly fitting dentures (need adjustment)
- Some adhesives contain zinc (long-term high doses can cause neurological issues)
- Doesn't restore palatal sensation
- Doesn't restore full biting force
Adhesive is a tool, not a fix. Properly fitting dentures shouldn't require constant adhesive. If your parent uses heavy adhesive, schedule a reline appointment.
Section 3: Recognition and Prevention (5 Questions)
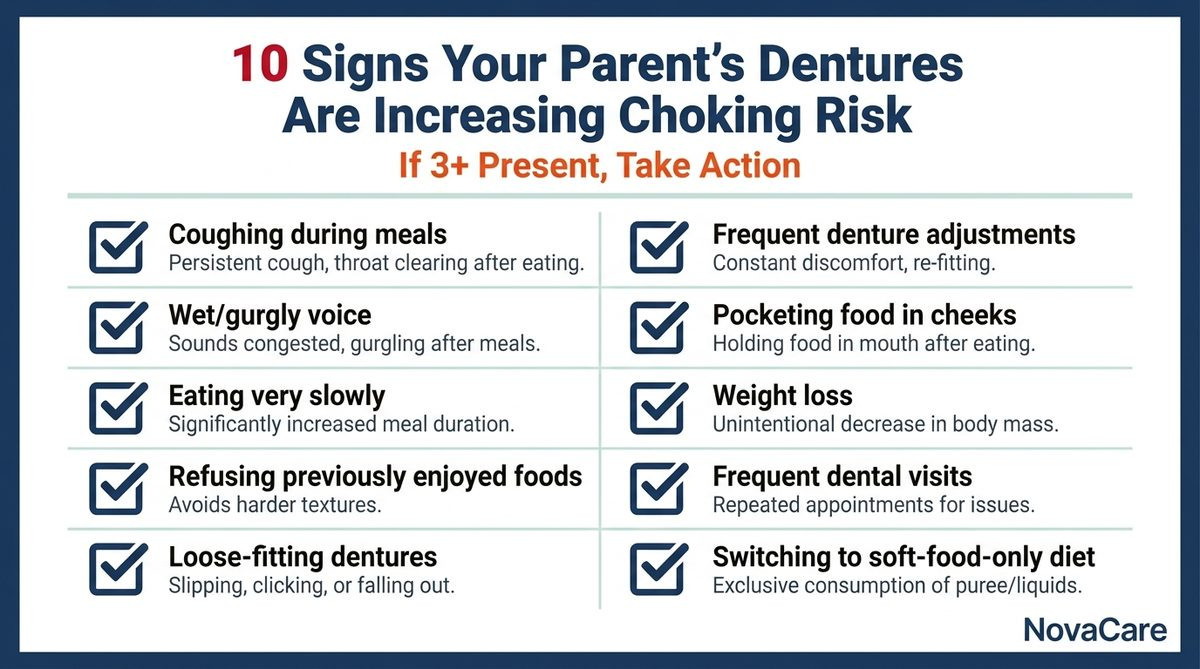
Q11: How do I know if my parent's dentures are increasing their choking risk?
Warning signs adult children should watch for:
- Coughing during or after meals — Often dismissed as "old age"
- Wet/gurgly voice after eating or drinking
- Eating very slowly — Compensating for reduced function
- Refusing previously enjoyed foods — Recognizing personal risk
- Loose-fitting dentures — Visible shifting
- Frequent denture adjustments — Sign of fit issues
- Pocketing food in cheeks — Inadequate chewing
- Weight loss — Reducing food intake from difficulty
- Dental visits more frequent — Adjustment chasing
- Switching to soft-food-only diet — Self-imposed restriction
If you notice 3+ of these signs, your parent's denture situation is creating elevated choking risk.
Q12: When should my parent see their dentist about their dentures?
Most denture wearers don't visit their dentist often enough. Recommended intervals:
- Annual check-up minimum (regardless of comfort)
- Reline every 3-5 years (gums shrink, dentures don't)
- New dentures every 5-10 years (materials wear out)
-
Immediate appointment if any of these occur:
- Sore spots persistent more than 1 week
- Dentures click or shift visibly
- Difficulty eating foods they used to enjoy
- Frequent breakage or repair
- Adhesive needed more than label specifies
Many seniors avoid dental visits due to cost, transportation, or inertia. Adult children may need to facilitate these appointments.
Q13: What dietary modifications help denture wearers?
Evidence-based modifications:
- Smaller bite sizes — Compensate for reduced biting force
- More moisture — Sauces, gravies, dipping
- Soft alternatives — Ground meat instead of steak
- Pre-cut foods — Reduce dependence on biting
- Slow eating pace — More time for proper chewing
- Adequate hydration — Reduces dry mouth
- Avoid talking while eating — Coordination already compromised
- Sit upright — Don't eat while reclined
These modifications maintain food enjoyment while dramatically reducing risk.
Q14: Should denture wearers avoid certain situations entirely?
High-risk situations to navigate carefully:
- Restaurant dining — Often have foods harder to chew, social pressure to eat normally
- Holiday family meals — Distraction, unusual foods, alcohol
- Buffet settings — Tempting to try too many foods quickly
- Eating while watching TV — Reduced attention to chewing
- Eating alone in routine — Habits develop without correction
- Drinking alcohol with meals — Compounds swallowing impairment
The goal isn't avoidance but awareness. These situations require more attention, smaller bites, and slower pace.
Q15: What about during the night — should dentures be removed?
YES — strongly recommended:
- Sleeping with dentures increases aspiration pneumonia risk significantly
- Per research, denture wearers sleeping with dentures have higher pneumonia hospitalization rates
- Gum tissue needs rest from constant pressure
- Reduces denture stomatitis (yeast infection under denture)
- Eliminates aspiration risk during sleep
The American Dental Association recommends removing dentures before sleep, cleaning them, and storing in water or denture solution overnight.
Many seniors resist this — feeling self-conscious about appearance or fearing they'll forget where they placed dentures. Storage cases beside the bed solve both problems.
Section 4: Equipment Preparedness for Denture Wearers (5 Questions)
Q16: Are denture wearers good candidates for anti-choking devices?
They're particularly good candidates. The reasons:
- Elevated baseline choking risk — Statistical reality
- Often older population — Compounding risk factors
- May live alone — Self-rescue capability essential
- Reduced cough effectiveness — Need mechanical assistance
- Often have other medical conditions — Multiple risk factors
- Heimlich may be more difficult — Osteoporosis, frailty
Anti-choking devices aren't optional safety equipment for denture wearers — they're essential complement to dental care.
Q17: Can someone use an anti-choking device with dentures in?
Yes, design considerations matter:
- Mask must seal around mouth (not require contact with teeth)
- Suction force must accommodate denture surfaces
- Operation must not require precise positioning by mouth
NovaCare's mask seals around lips and chin, not requiring contact with teeth or dentures. The 70 kPa suction (verified by Bureau Veritas, Report BV2500728QN7119) is sufficient to dislodge obstructions even with dentures in place.
Note: in some cases, the suction may dislodge poorly-fitting dentures along with the obstruction. This is typically a benefit (clear airway completely), not a problem.
Q18: How does NovaCare compare to other devices for denture wearers?
| Device | Status | For Denture Wearers |
|---|---|---|
| LifeVac | FDA De Novo Authorized (March 2026) | Bystander-administered, single-use, two-handed plunger |
| NovaCare | Bureau Veritas Tested | Self-rescue capable, reusable, one-button mechanical |
| Sonmol | Various certifications | Wall-mounted, 5-step operation |
| Dechoker | Multiple FDA actions | Tube-based, more complex |
For a denture-wearing senior living alone, self-rescue capability is essential. NovaCare's design specifically accommodates this scenario.
Q19: Where should denture-wearing seniors keep equipment?
Strategic placement:
- Kitchen counter — Most eating happens here
- Dining table area — Backup primary location
- Bedside table — In case denture aspiration during night
- Bathroom counter — When removing dentures
- Travel bag — Restaurants, vacations
For denture wearers who travel or socialize frequently, a portable device is crucial. NovaCare's 16cm size fits in standard handbags and travel bags.
Q20: What about practice with dentures?
Family practice considerations:
- Demonstrate device with senior's actual denture configuration
- Practice positioning that doesn't disturb dentures
- Verify mask seal works with their specific mouth shape
- Test with both upper and lower dentures in
- Discuss what to do if dentures dislodge during use
This eliminates the "what if my dentures fall out" anxiety that might cause hesitation in a real event.
Section 5: The Adult Children's Action Framework (5 Questions)
Q21: How do I bring this up with my parent without offending them?
Sensitive conversation approaches:
Frame as research, not concern about them:
- "I read an article about dentures and choking risk — interesting research"
- "Did you know they did studies showing denture wearers have different swallowing?"
- "There's actually peer-reviewed data on this"
Reference your own preparation:
- "We got an anti-choking device for our house. Thought you might want one too."
- "This is becoming standard for our generation."
Acknowledge their independence:
- "You're fully capable — I just want you to have tools to stay that way."
- "This isn't about you being fragile, it's about being prepared."
Avoid:
- "You're getting older so..."
- "Mom, you really should..."
- "Dad, your teeth aren't real anymore..."
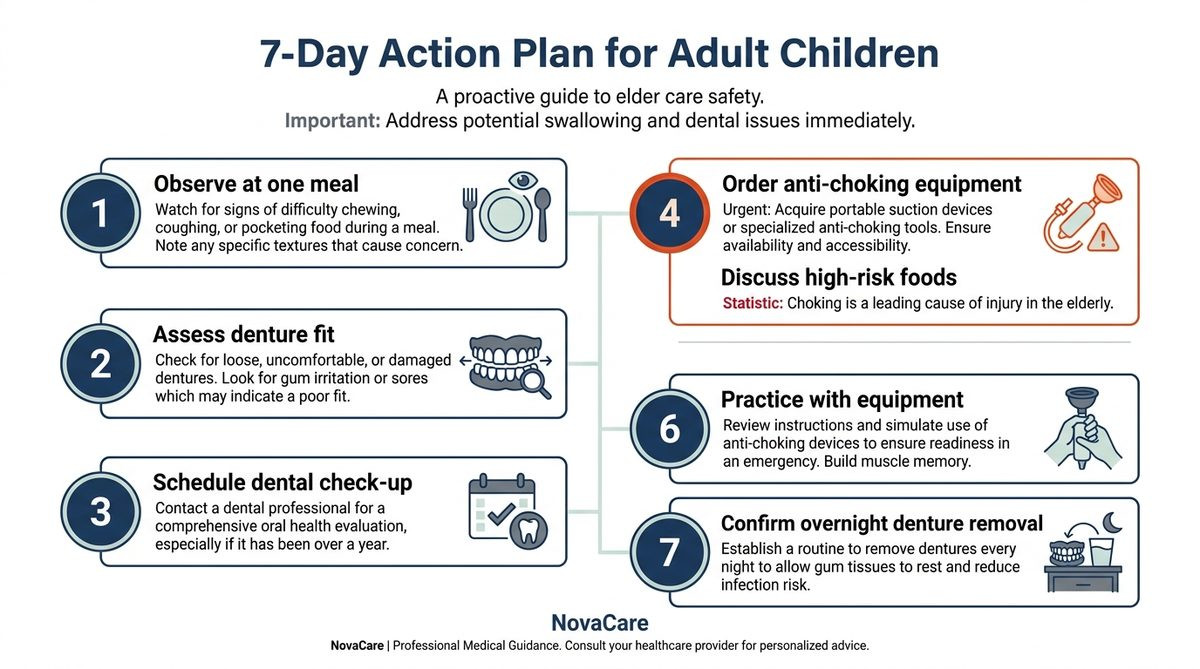
Q22: What should be the first thing I do?
Within 7 days:
- Observe at one meal — Watch for warning signs (Q11)
- Assess denture fit — Loose? Clicking? Frequent adjustment?
- Schedule dental check-up — Especially if dentures are 3+ years since reline
- Order anti-choking equipment — NovaCare 2-pack covers home + travel
- Discuss high-risk foods — Awareness without restriction
- Practice with equipment — Family session
- Confirm overnight denture removal — Aspiration prevention
This sequence addresses the highest-leverage interventions first.
Q23: What if my parent gets new dentures soon?
New dentures actually represent both opportunity and risk:
Opportunities:
- Better fit reduces immediate risk
- Modern materials offer improved chewing
- Optimization for individual anatomy
- Chance to discuss safety concerns with dentist
Initial risks:
- Adaptation period (typically 30-60 days)
- Increased gag reflex initially
- Speech and eating patterns disrupted
- May try foods inappropriate for new dentures
- Confidence may exceed actual capability
For seniors with new dentures, the first 60 days are particularly high-risk. Equipment readiness during this period is essential. Modified diet during adaptation reduces risk significantly.
Q24: How does this connect to medications my parent takes?
Critical compounding factor — see our complete drug-induced choking guide.
Many seniors on dentures also take medications that further compromise swallowing:
- Anticholinergics → severe dry mouth, worsens denture fit
- Antipsychotics → dopamine effects on swallowing
- Benzodiazepines → sedation during meals
- Sleep aids → confusion + dentures = aspiration during sleep
The combination of dentures + multiple medications creates exponentially higher risk than either alone. Medication review using AGS Beers Criteria is essential.
Q25: What's the most important thing to remember?
One core insight: your parent's dentures aren't just replacing teeth — they're altering swallowing mechanics in measurable ways.
This isn't a minor issue or theoretical risk. Peer-reviewed research documents:
- Reduced oral sensation
- Impaired swallowing function (videofluoroscopic evidence)
- Reduced lung function (2.37x airflow limitation risk)
- Reduced chewing capacity (75-85% biting force loss)
Combined with normal age-related changes, the result is significantly elevated choking risk that most families never discuss.
The intervention: awareness + dental optimization + equipment readiness + dietary modification = dramatically reduced actual risk for denture-wearing parents.
For Adult Children: A Letter to You
Your parent wears dentures.
Maybe they got them ten years ago after losing teeth. Maybe they've worn full dentures since their 60s. Maybe they have partial dentures with metal clasps. The specific configuration matters less than this fact: their swallowing mechanics have been measurably altered.
The dental industry tends to focus on cosmetics and chewing capability. Eating again normally after tooth loss is wonderful — but it comes with hidden complications most denture wearers never hear about.
You can change this for your family:
This week, watch them eat one meal. Listen for the wet voice afterward. Note if they're avoiding foods they used to love. Check whether their dentures fit properly or click while talking.
Next week, take them to their dentist. Reline if it's been 3+ years. Ask specifically about palatal sensation and swallowing — most dentists won't volunteer this discussion.
The week after, get anti-choking equipment in their home. The same equipment that saved Harold B. (Save #156, choked on steak alone) and Dorothy F. (Save #162, choked on hard candy alone) — both denture-aged seniors who survived because the device was within reach and operable solo.
Adult children of denture-wearing parents have a specific responsibility that most families never discuss. Your parent's dentures have been altering their swallowing for years. Equipment readiness completes what dental care started.
→ Get NovaCare for Your Denture-Wearing Parent — $63.98 single · $119.98 2-pack
The 2-pack covers their home + your home for visits.

The Bottom Line
Dentures dramatically increase choking risk through reduced oral sensation, impaired swallowing function (videofluoroscopic evidence), reduced biting force (75-85% loss vs natural teeth), and reduced cough capacity (2.37x airflow limitation risk per PRIME study). With ~40 million American denture wearers, most over 65, this represents an enormous under-discussed risk population. Adult children need to address denture fit, dietary modifications, and equipment readiness — not just dental cosmetics.
- ✅ Bureau Veritas Tested (Report BV2500728QN7119)
- ✅ 70 kPa Medical-Grade Suction (Independently Verified)
- ✅ IP65 Rated (Dust & Water Resistant)
- ✅ CE & UKCA Certifications In Progress
- ✅ 20 Documented Saves in 2026
- ✅ 2 Senior Self-Rescues (#156, #162)
- ✅ Reusable Design (Not Single-Use)
- ✅ Mechanical One-Button (No Batteries)
- ✅ Self-Rescue Capable
- ✅ $63.98 single · $119.98 2-pack
- ✅ Free US Shipping
- ✅ 90-Day Money-Back Guarantee
→ Get NovaCare at novacareus.com
📖 Related: Anti-Choking Device for Seniors: 30 Questions Answered
📖 Related: Drug-Induced Choking: Senior Medications
📖 Related: Choking While Alone: Solo Senior Safety
📖 Related: Aspiration Pneumonia in Seniors
📖 Related: NovaCare 2026 Lives Saved Report